Can Left Ventricular Rotational Function Compensate For Marked Impairment In Longitudinal Strain In Early Cardiac Amyloidosis?
Cristiane Singulane, Jeremy A. Slivnick, Karima Addetia, Federico M. Asch, Victor Mor-Avi, Roberto M. Lang
Background
- Studies have shown that cardiac amyloidosis (CA) involvement typically begins in the subendocardium where longitudinal fibers are predominantly located.
- Until the advanced stages of CA, left ventricular ejection function (LVEF) is typically preserved, despite the coinciding impairment in global longitudinal strain (GLS).
- We hypothesized that this discrepancy at earlier stages of CA could be explained by preservation or compensatory augmentation of circumferential strain (GCS).
Methods
- 67 patients with proven CA (29 with LVEF>50% and 38 with LVEF<50), who had undergone surface echocardiogram, were identified.
- Speckle tracking was used to measure GLS from the 3 long-axis views, and GCS from basal, mid, and apical short-axis slices (Tomtec).
- Impairment in GCS and GLS was defined by strain magnitudes below the 97.5th percentile (lower limit of normal) for subjects from the WASE study, after excluding subjects with inadequate image quality or those lacking appropriate short axis sequences (N=160/2008).
- Global GLS and GCS, as well as basal, mid, and apical GCS were compared between CApEF and CArEF groups.
- The relationship between both strains and 5-year mortality was assessed using univariate Cox regression analysis.
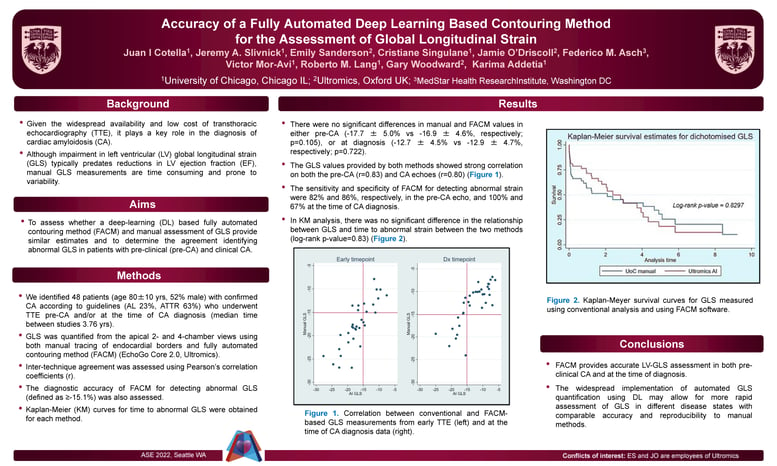
Results
- Strain measurements for both cohorts, including CApEF and CArEF subgroups, are shown in Table 1.
- Impaired GCS was present in 36(95%) of CArEF patients compared with 4(14%) of CApEF (p<0.0001, Figure 3).
- Impaired GLS was present in 100% of patients in both groups irrespective of LVEF without significant intergroup differences.
- Both GLS and GCS were significantly more impaired in the CArEF compared to CApEF (Table 1).
- Both GCS (HR 1.047 [1.007-1.088], p=0.021) and GLS (HR 1.163 [1.052-1.285] p=0.003) were
Conclusion
The early predilection of CA towards the sub-endocardium (longitudinal fibers-GLS) rather than the mid myocardium (circumferential fibers-GCS) is the likely reason why GCS is frequently normal early in the course of CA, resulting in temporary preservation of LVEF, despite marked impairment in GLS.
At more advanced stages of the disease, both GLS and GCS magnitudes are reduced resulting in reduced LVEF.