Using AI to make precision heart failure detection possible

Up to 75% of heart failure patients are missed. 1
High rates in missed cases are associated with an increase in hospitalizations, high readmission rates, unnecessary procedures, and often death.
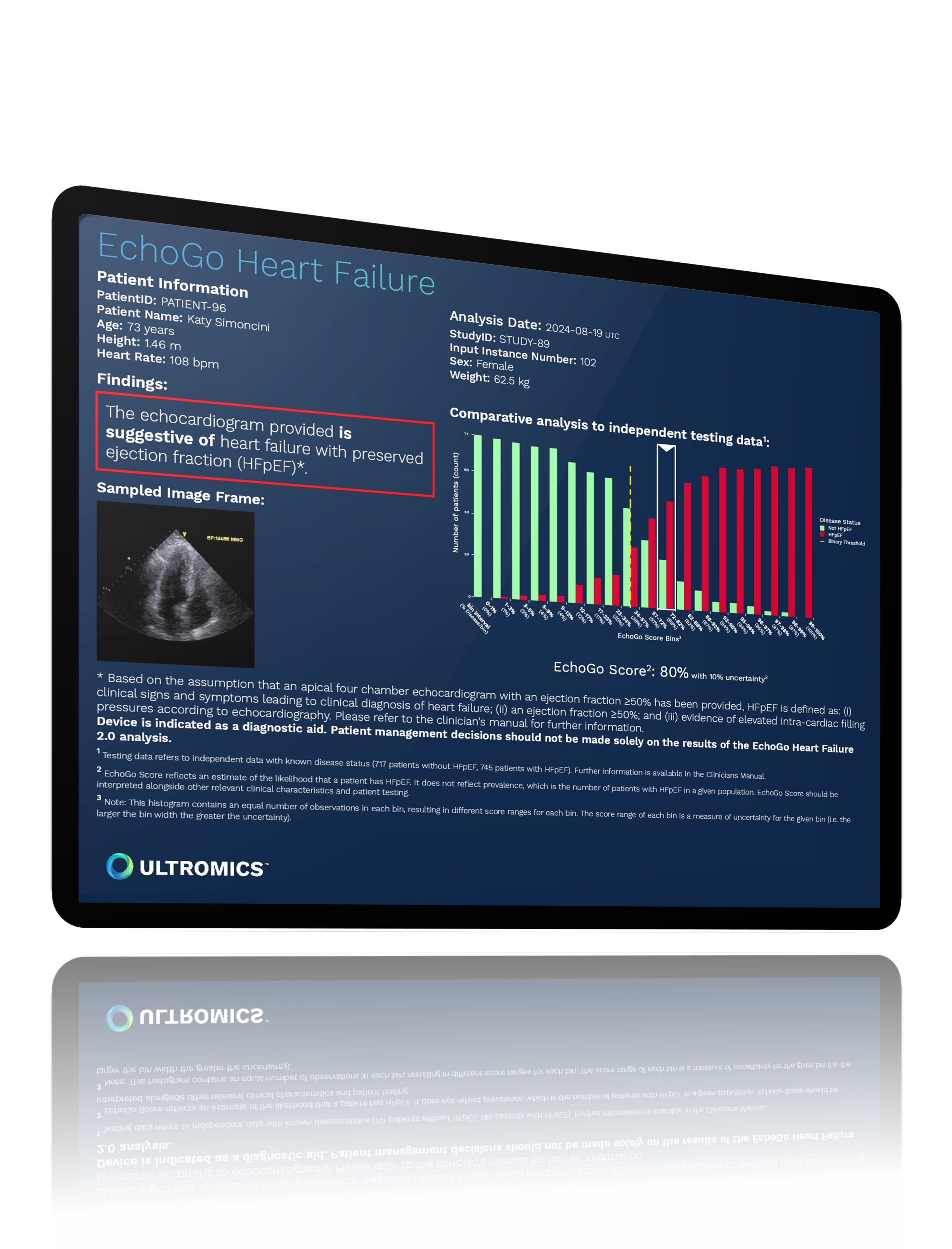
To improve and extend lives, and decrease associated costs, we need to detect heart failure earlier and more accurately. This is especially true for patients with heart failure with preserved ejection fraction (HFpEF).

Precision heart failure detection
Ultromics combines echocardiography - the most common and cost-effective cardiac imaging modality - with AI-derived insights that go beyond what the human eye can detect.
Ultromics’ AI specializes in early and accurate heart failure detection and risk stratification, including HFpEF, to reduce hospitalizations and help improve patient outcomes.

$25,000
The annual median medical costs for heart failure care per patient.2

80%
The number of direct heart failure costs attributed to inpatient stays.
> 3 million
#1 driver
More focus needed on HFpEF
Heart failure with preserved ejection fraction (HFpEF) is the single greatest unmet need in cardiovascular medicine. [3]
HFpEF is more costly than the more commonly diagnosed heart failure with reduced ejection fraction (HFrEF) and represents a greater proportion of heart failure costs. [4]
HFpEF diagnosis is complex and replies on often inconclusive diagnostic algorithms and invasive testing – such as catheterization – which contributes to it being missed up to 75% of the time. [1]



AI-driven insights consistently deliver accurate, reproducible results that reduce the costs associated with rehospitalization and invasive procedures.