Automated Analysis Of Segmental Longitudinal Strain In Ischemic Heart Disease
William Hawkes, Ashley Akerman, Tine Deschamps, Andrew Parker, Jamie O’Driscoll, Rajan Sharma, Gary Woodward
Background
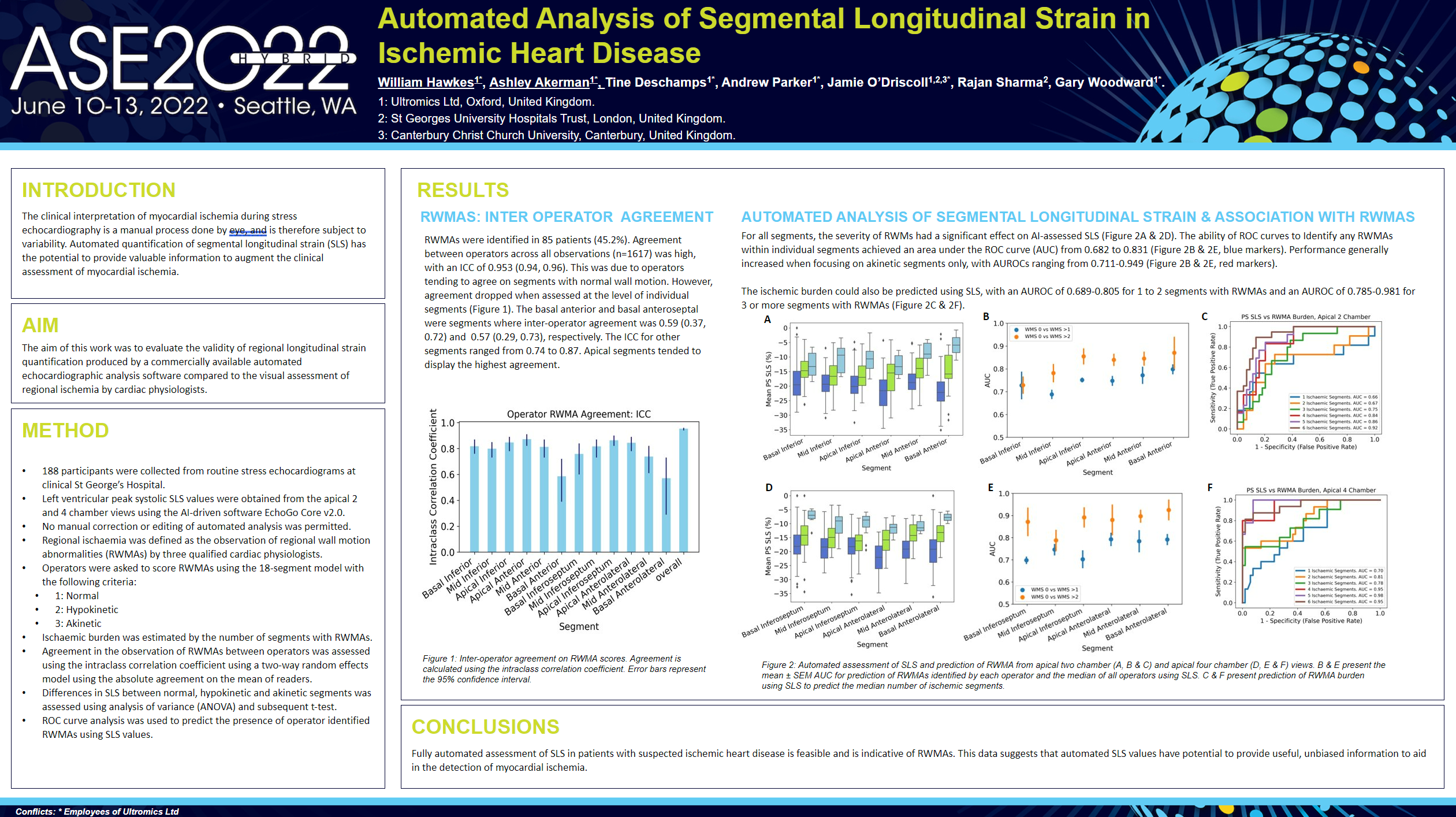
The clinical interpretation of myocardial ischemia during stress echocardiography is a manual process done by eye, and is therefore subject to variability. Automated quantification of segmental longitudinal strain (SLS) has the potential to provide valuable information to augment the clinical assessment of myocardial ischemia.
Methods
- 188 participants were collected from routine stress echocardiograms at clinical St George’s Hospital.
- Left ventricular peak systolic SLS values were obtained from the apical 2 and 4 chamber views using the AI-driven software EchoGo® Core v2.0.
- No manual correction or editing of automated analysis was permitted.
- Regional ischaemia was defined as the observation of regional wall motion abnormalities (RWMAs) by three qualified cardiac physiologists.
Operators were asked to score RWMAs using the 18-segment model with the following criteria:
1: Normal
2: Hypokinetic
3: Akinetic - Ischaemic burden was estimated by the number of segments with RWMAs.
- Agreement in the observation of RWMAs between operators was assessed using the intraclass correlation coefficient using a two-way random effects model using the absolute agreement on the mean of readers.
- Differences in SLS between normal, hypokinetic and akinetic segments was assessed using analysis of variance (ANOVA) and subsequent t-test.
- ROC curve analysis was used to predict the presence of operator identified RWMAs using SLS values.
Results
RWMAs were identified in 85 patients (45.2%). Agreement between operators across all observations (n=1617) was high, with an ICC of 0.953 (0.94, 0.96). This was due to operators tending to agree on segments with normal wall motion. However, agreement dropped when assessed at the level of individual segments (Figure 1). The basal anterior and basal anteroseptal were segments where inter-operator agreement was 0.59 (0.37, 0.72) and 0.57 (0.29, 0.73), respectively. The ICC for other segments ranged from 0.74 to 0.87. Apical segments tended to display the highest agreement.
Conclusion
Fully automated assessment of SLS in patients with suspected ischemic heart disease is feasible and is indicative of RWMAs. This data suggests that automated SLS values have potential to provide useful, unbiased information to aid in the detection of myocardial ischemia.