Association Of A Novel, Non-Invasive AI Model To Automate Echocardiographic Detection Of Heart Failure With Preserved Ejection Failure (HFpEF) With Invasive Hemodynamics
Hamid, H,MD1, Fudim, M, MD2, Laufer-Pearl, M, MD3, Alenezi, F, MD2, Upton, R, PhD4, Akerman, A, PhD4, Shaburishviili, T, MD5
1Allina Health Minneapolis Heart Institute, Minneapolis, MN, 2Duke University, Durham, NC, 3Tel Aviv, Sourasky Medical Center, Tel Aviv, Israel, 4Ultromics Ltd, Oxford, UK, 5Tbilisi Heart and Vascular Clinic, Tbilisi, Georgia
Background
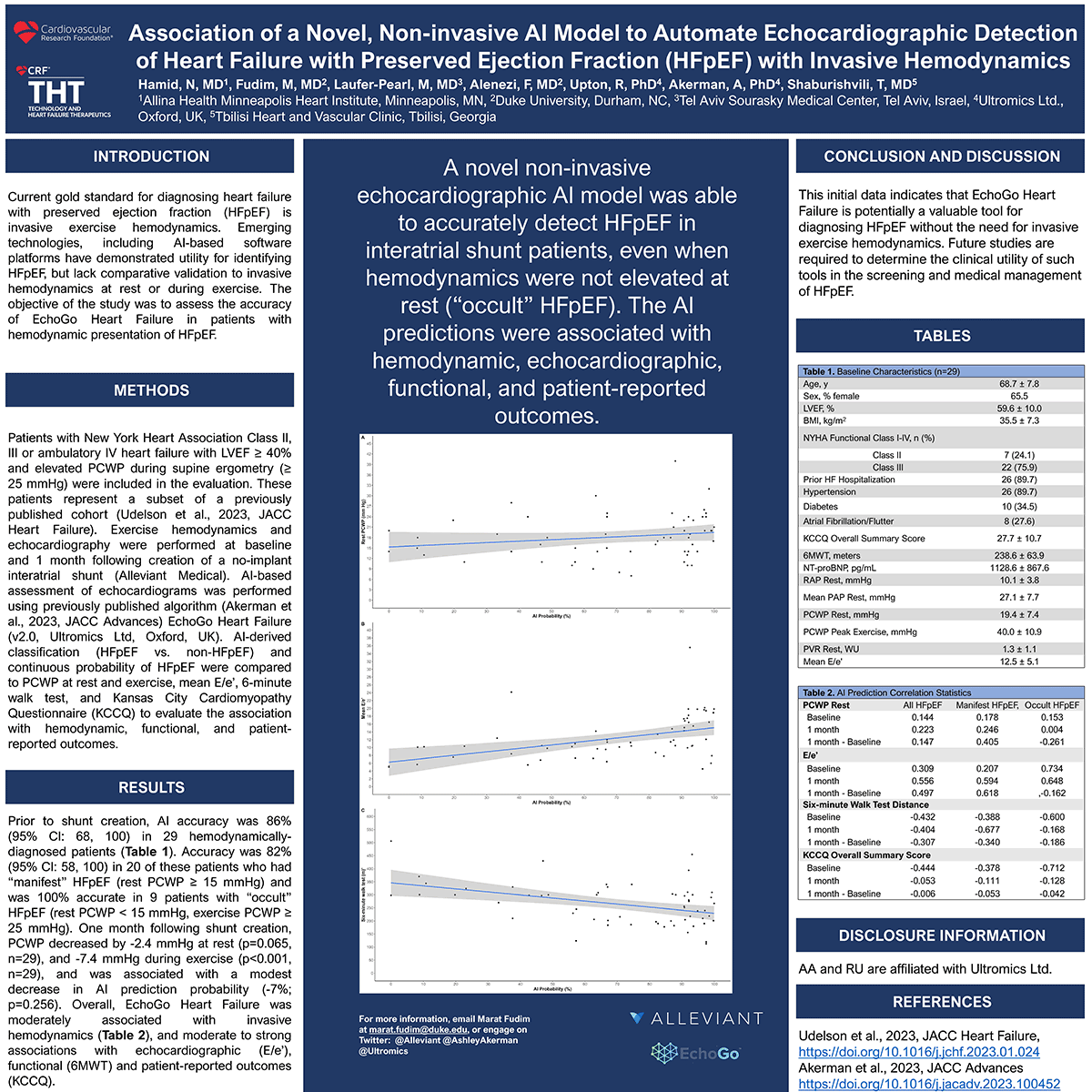
Current gold standard for diagnosing heart failure with preserved ejection fraction (HFpEF) is invasive exercise hemodynamic. Emerging technologies, including Al-based software platforms have demonstrated utility for identifying HFpEF, but lack comparative validation to invasive hemodynamic at rest or during exercise. The objective of the study was to assess the accuracy of EchoGo® Heart Failure in patients with hemodynamic presentation of HFpEF.
Methods
Patients with New York Heart Association Class 11, Ill or ambulatory IV heart failure with LVEF 40% and elevated PCWP during supine ergometry (2'25 mmHg) were included in the evaluation. These patients represent a subset of a previously published cohort (Udelson et al., 2023, JACC Heart Failure). Exercise hemodynamics and echocardiography were performed at baseline and 1 month following creation of a no-implant interatrial shunt (Alleviant Medical). Al-based assessment of echocardiograms was performed using previously published algorithm (Akerman et al., 2023, JACC Advances) EchoGo Heart Failure (v2.0, Ultromics Ltd, Oxford, UK). Al-derived classification (HFpEF vs. non-HFpEF) and continuous probability of HFpEF were compared to PCWP at rest and exercise, 6-minute walk test, and Kansas City Cardiomyopathy Questionnaire (KCCQ) to evaluate the association with hemodynamic, functional, and patient-reported outcomes.
Results
Prior to shunt creation, Al accuracy was 86% (95% Cl: 68, 100) in 29 hemodynamicallydiagnosed patients (Table 1). Accuracy was 82% (95% Cl: 58, 100) in 20 of these patients who had "manifest" HFpEF (rest PCWP 2' 15 mmHg) and was 100% accurate in 9 patients with "occult" HFpEF (rest PCWP < 15 mmHg, exercise PCWP ;25 mmHg). Following shunt creation, PCWP decreased at rest (-2.4 mmHg; p=0.065, n=29) and during exercise (-7.4 mmHg; p<0.001, n=29). Al probability decreased slightly (-7%; p=0.256), and while weaker associations were evident in invasive hemodynamics (Table 2), moderate to strong relations were observed with echocardiographic (E/e') and functional (6MWT) and patient-reported outcomes.
Conclusion
This initial data indicates that EchoGo Heart Failure is potentially a highly valuable tool for diagnosing HFpEF without the need for invasive exercise hemodynamics. Future studies are required to determine the clinical utility of such tools in the screening and medical management of HFpEF.